
Small intestinal bacteria overgrowth (SIBO) may be more prevalent than we think. Research shows that 50-84% of IBS patients test positive for SIBO. This is with old testing methods that would show many false positives, therefore my assumption is that it is even more prevalent than we think. All it may take for someone to develop SIBO is a bout of food poisoning! That’s it! For some it is more complicated than that.
I have discussed the main reasons someone may have SIBO in a previous post, but let’s jump right into how you accurately diagnose SIBO. In my practice I ask a lot of questions in the first visit. This is because we can gain a lot of clinical information about what may be going on by just getting all the information. A physical exam, specifically an abdominal exam in these cases, is my next step in gathering information. SIBO has a handful of specific symptoms I am looking for which guide my treatment plan. But SIBO also a handful of symptoms that are unique to the individual and can be systemic, for example joint pain, rosacea, hypothyroidism.
Test Don’t Guess
If your symptoms indicate to me that you may have SIBO, before jumping into treatment, it is very helpful to test for it. Not only will this confirm, or deny, a positive result, but it will also guide what type of antimicrobials I’ll use and for how long depending on what the results show. The higher the results, the more rounds of antimicrobials we typically have to do.
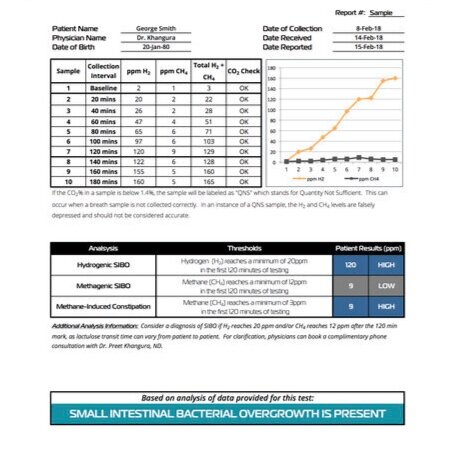
The SIBO breath test is the most accurate non-invasive way to diagnose SIBO right now. Research continues to be done to advance our testing methods. The best option is a breath test that is a 3-hour lactulose breath test looking at both Hydrogen (H2) and methane (CH4) levels. This is the type and amount of gas that is produced if you have SIBO. Hydrogen SIBO typically presents as diarrhea (among other symptoms), and methane SIBO typically presents as constipation. The 3 hour test ensures you are testing the entire length of the small intestine, where only a small amount of bacteria should be, not an overgrowth. Stool testing, which we may do for other GI complaints, is only relevant to the large intestine. There is no accurate test yet for a 3rd type of SIBO, hydrogen sulphide. However, there are patterns on the results and patterns in symptoms that may indicate this type. This is not testing for Candida, however it is common for these to present together.
Ultimately if you test positive for SIBO, I treat it. However, 2/3 of patients have shown to relapse post-treatment. There are number of reasons for this but this is why it is always important to treat the patients and not the condition. I aim to treat the root cause along with the SIBO - if we can. Sometimes this isn’t possible depending on the case, so we do are best. It can also take time, and even different circumstances, for example a less stressful job perhaps, to treat the root. 1/3 of cases are luckily non-recurring and the patients feels better quickly and for good. Phew!
All in all, testing is very helpful to me as a clinician if I suspect a bad case of SIBO. It takes the guesswork out of the treatment and ensures a more accurate and quicker treatment result. Treating SIBO is a team effort but the more information we have the better it can be!
Are you interested in getting tested for SIBO? Let me know!
In health & happiness,
Dr. Karen